
Androgenetic alopecia (AGA) is a genetically mediated, androgen-dependent, progressive miniaturization of scalp hair follicles characterized by patterned hair thinning in men and women. It results from increased follicular sensitivity to dihydrotestosterone (DHT), shortened anagen (growth) phases, and gradual conversion of terminal hairs into fine vellus-like hairs. In 2026, management focuses on early diagnosis, DHT modulation, follicular stimulation, regenerative therapies, and precision-based treatment algorithms tailored to individual hormonal, genetic, and inflammatory profiles.
As a clinician specializing in hair disorders, I routinely explain to patients that AGA is not simply cosmetic it is a chronic, biologically active condition requiring longitudinal management. Modern therapy aims to stabilize progression, reverse miniaturization where possible, and maintain scalp health using multimodal interventions.
Androgenetic Alopecia in 2026: Pathophysiology and Clinical Classification
The year 2026 marks a significant shift toward molecular-level understanding of AGA. While DHT remains central, research now highlights perifollicular microinflammation, oxidative stress, prostaglandin imbalance, and follicular stem cell niche dysfunction as co-contributors.
Hormonal and Genetic Mechanisms
DHT, derived from testosterone via 5-alpha-reductase (types I and II), binds to androgen receptors in susceptible hair follicles. In genetically predisposed individuals, this triggers:
.1 Progressive shortening of the anagen phase
. Prolongation of telogen
. Follicular miniaturization
.Reduced dermal papilla size
.Decreased hair shaft diameter
Genome-wide association studies updated through 2025 confirm polygenic inheritance involving androgen receptor (AR) gene polymorphisms and regulatory loci affecting follicular cycling pathway.
Clinical Patterns
Men typically present with frontotemporal recession and vertex thinning (Norwood-Hamilton scale). Women more often exhibit diffuse central thinning with preserved frontal hairline (Ludwig scale).
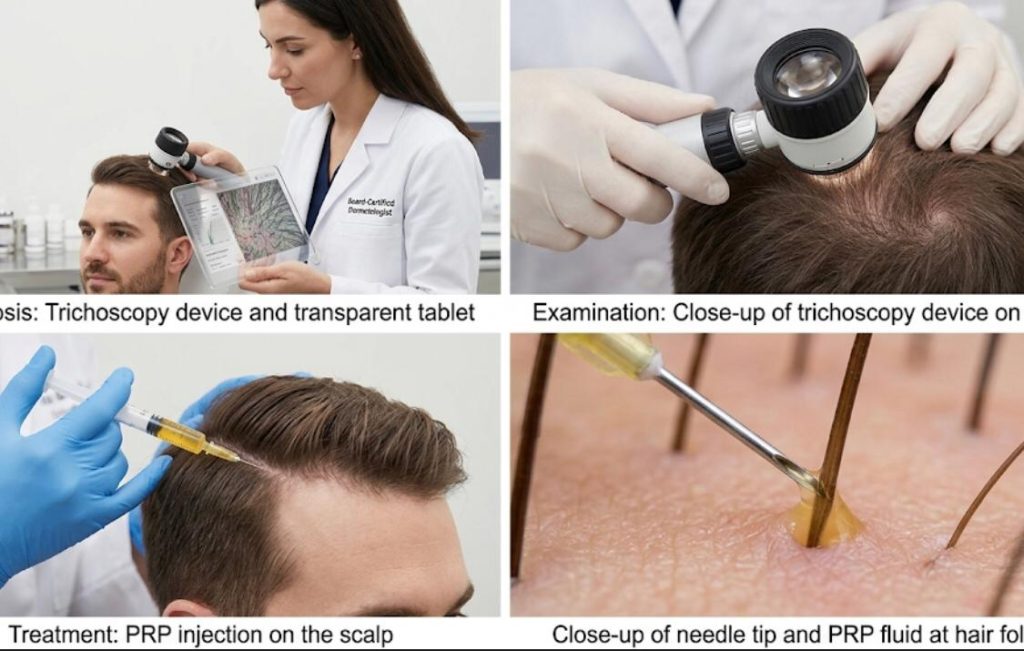
Trichoscopy in 2026 includes AI-assisted follicular density mapping, quantifying:
– Hair shaft diameter variability (>20% suggests AGA)
– Perifollicular erythema
– Miniaturized follicle clusters
Digital scalp imaging now integrates predictive modeling to estimate projected progression over 5–10 years.
Foundational Pharmacologic Strategies
Pharmacologic therapy remains first-line in 2026, particularly when initiated early.
DHT Suppression
DHT reduction slows follicular miniaturization. 5-alpha-reductase inhibitors reduce conversion of testosterone to DHT, with measurable scalp DHT reduction within weeks.
Precision Medicine Approach to AGA
Modern AGA treatment is algorithm-driven and individualized.
Hormonal Profiling
In 2026, baseline testing may include:
– Serum testosterone
– DHT levels
– SHBG (sex hormone binding globulin)
– Thyroid panel
– Ferritin
Women with suspected hyperandrogenism undergo additional endocrine evaluation.
This allows clinicians to estimate response probability to specific therapies.
PRP remains a cornerstone adjunctive therapy. Modern protocols utilize:
– Double-spin centrifugation
– Leukocyte-poor preparations
– Injection every 4–6 weeks for 3 sessions
PRP enhances follicular stem cell signaling and prolongs anagen.
Exosome Therapy
Exosome-based scalp injections, derived from mesenchymal stem cells, are under expanded clinical use in 2026. These nano-vesicles contain growth factors and signaling proteins that influence follicular regeneration.
Low-Level Laser Therapy (LLLT)
Surgical Strategies: Hair Transplantation in 2026
Hair transplantation remains definitive for advanced AGA.
Follicular Unit Extraction (FUE)
Robotic-assisted FUE increases graft survival rates and reduces transection. AI mapping identifies optimal donor zones.
Medication Allocation Section
Propecia (finasteride 1mg) remains a first-line oral therapy for male androgenetic alopecia, reducing scalp DHT and slowing miniaturization with daily dosing under physician supervision.
Proscar (finasteride 5mg) is sometimes prescribed off-label in adjusted dosing regimens when clinically appropriate, while Avodart (dutasteride) offers dual inhibition of type I and II 5-alpha-reductase and may be considered in select, carefully monitored patients.
Safe Procurement and Authentic Treatment Access
Obtaining authentic pharmacologic therapy requires medical oversight. Patients must consult licensed physicians before initiating DHT-modulating medications, as hormonal effects require evaluation and follow-up monitoring.
Counterfeit hair loss medications remain a serious concern in global e-commerce markets. Laboratory analyses published between 2023–2025 revealed that non-accredited online vendors frequently distribute subtherapeutic or contaminated products.
When patients choose to buy, purchase, order, or secure prescription treatments, they should:
– Use verified, accredited pharmacies
– Confirm state or national licensing
– Avoid websites offering prescription drugs without medical evaluation
– Request manufacturer verification if uncertain
Board-certified dermatologists and hair restoration specialists coordinate prescriptions through secure online pharmacy networks to ensure authenticity and safety.
In my clinical practice, I routinely review pharmacy sourcing with patients. Those who previously obtained medication through informal channels often present with inconsistent therapeutic responses.
Combination Therapy: The Modern Standard
Monotherapy rarely produces optimal long-term outcomes. Most 2026 treatment plans combine:
– DHT suppression
– Follicular stimulation
– Regenerative adjuncts
– Lifestyle optimization
Lifestyle Factors
Sleep, stress modulation, smoking cessation, and micronutrient sufficiency significantly affect hair cycling biology.
Nutritional Considerations
Low ferritin (<40 ng/mL) impairs hair growth. Vitamin D insufficiency correlates with increased telogen shedding.
Monitoring and Long-Term Follow-Up
AGA requires structured monitoring:
– Digital scalp imaging every 6 months
– Hair density counts
– Patient-reported outcome measures
Treatment adjustments are data-driven rather than anecdotal.
I advise patients to view therapy as long-term maintenance, similar to managing hypertension. Discontinuation often results in resumed progression within 6–12 months.
Future Directions in AGA Management
Research pipelines in 2026 include:
.Wnt pathway modulators
.JAK-STAT pathway regulators
.Hair follicle cloning
.Topical gene therapy vectors
Although not yet standard of care, these innovations may redefine treatment paradigms within the next decade.
Advanced Follicular Biology: What We Understand in 2026
The hair follicle is now recognized as a highly dynamic mini-organ with immune privilege characteristics. In AGA, this immune privilege becomes partially disrupted.
Perifollicular Microinflammation
Scalp biopsies in progressive AGA frequently demonstrate:
.Mild lymphocytic infiltrates
.Increased prostaglandin D2 (PGD2) levels
.Oxidative stress markers
.Collagen deposition around follicles
This inflammatory microenvironment contributes to miniaturization. In 2026, anti-inflammatory modulation has become a secondary therapeutic pillar.
Bulge-area stem cells remain present even in advanced AGA, but their signaling capacity declines. This discovery reshaped treatment philosophy. The follicle is not destroyed it is suppressed.
Therapies now aim to reactivate dormant regenerative signaling rather than merely blocking hormones.
Advanced Pharmacologic Adjuncts
Low-Dose Oral Minoxidil (LDOM)
Low-dose oral minoxidil has gained substantial clinical acceptance. Unlike topical formulations, systemic administration improves adherence and ensures consistent follicular exposure.
Typical dosing range (2026 protocols):
– Men: 1.25–5 mg daily
– Women: 0.25–2.5 mg daily
Monitoring includes:
– Blood pressure assessment
– Baseline cardiovascular review
– Edema evaluation
– Combined with topical growth stimulants
Surgical Planning: Advanced 2026 Considerations
Hair transplantation is no longer simply about graft placement density.
Donor Area Mapping
High-resolution AI-assisted donor scanning evaluates:
– Follicular unit density
– Hair caliber
– Donor depletion risk modeling
– Long-term safe harvest calculations
This prevents overharvesting and future aesthetic imbalance.
Robotic-Assisted FUE
Robotic systems in 2026 feature:
– Real-time transection detection
– Automated angle correction
– Machine-learning-guided punch selection
Graft survival rates now routinely exceed 90% in experienced centers.
Recipient Site Engineering
Implantation density must consider:
– Native hair miniaturization
– Long-term progression patterns
– Future transplant planning
Aggressive frontal packing without stabilizing therapy often produces unsustainable results.-
Female Pattern Hair Loss (FPHL): Distinct 2026 Strategies
Female AGA requires careful differentiation from:
– Telogen effluvium
– Chronic diffuse alopecia
– Autoimmune causes
Hormonal Evaluation
Women may require assessment for:
– Polycystic ovarian syndrome (PCOS)
– Elevated androgens
– Iron deficiency
– Thyroid dysfunction
Treatment often includes:
– Low-dose oral minoxidil
– Spironolactone
– Topical therapy combinations
Pregnancy considerations significantly influence medication choices.
Psychodermatology: The Emotional Component
Hair loss carries measurable psychological burden. Studies published between 2023–2025 confirm:
– Increased anxiety prevalence
– Higher rates of body image distress
-I routinely schedule extended consultations for younger patients experiencing rapid progression. The reassurance provided during early intervention often changes long-term emotional outcomes.
Seborrheic Dermatitis Control
Inflammatory scalp conditions accelerate shedding. Antifungal shampoos containing ketoconazole (2%) are widely integrated into regimens.
Ketoconazole also demonstrates mild antiandrogen properties at the follicular level.
Oxidative Stress Mitigation
Topical antioxidants and polyphenol-based serums are emerging adjuncts aimed at reducing reactive oxygen species in perifollicular tissue.
Long-Term Maintenance Strategy
AGA management requires a maintenance framework:
1. Initial stabilization (6–12 months)
2. Density optimization (12–24 months)
3. Long-term preservation phase
Stopping therapy typically results in gradual reversion to the natural progression pattern.
Special Populations
Young Men (Under 25)
Early intervention prevents extensive miniaturization. Conservative transplant planning is mandatory due to unpredictable long-term progression.
Aging Patients
Hair caliber naturally declines with age. Treatment intensity may be adjusted to reflect realistic density goals.
Emerging Research Frontiers
Wnt Signaling Activation
Wnt pathway stimulation is a major research focus. Topical modulators targeting this pathway may promote follicular neogenesis.
Hair Cloning and Follicular Multiplication
Laboratory-based follicular cell expansion techniques are in early clinical development stages. Widespread availability is not yet established.
JAK-STAT Modulators
Although primarily studied in alopecia areata, pathway modulation research is expanding into patterned hair loss biology.- Stabilized frontal recession
Nutritional and Lifestyle Interventions
Iron and Ferritin
Ferritin levels below 40 ng/mL impair anagen maintenance. Supplementation protocols are individualized.
Vitamin D
Suboptimal vitamin D correlates with increased shedding. Correction improves follicular cycling stability.
Stress and Cortisol
Chronic stress influences telogen transition. Sleep hygiene and stress-reduction strategies support medical therapy.
Monitoring Metrics in 2026
Modern tracking includes:
– Hair density (hairs/cm²)
– Terminal-to-vellus ratio
– Hair shaft diameter measurement
– AI progression modeling
Patients appreciate objective data. It reduces reliance on subjective mirror assessment.
Realistic Outcome Counseling
Complete restoration of adolescent density is rarely achievable in advanced AGA. The objective is visible improvement and long-term stability.
Overpromising remains one of the greatest risks in hair restoration practice.
Advanced Therapeutic Algorithms and Emerging Modalities (2026 Expansion)
The management of androgenetic alopecia (AGA) in 2026 extends far beyond first-line pharmacology and standard hair transplantation. What distinguishes high-level hair restoration practices today is structured, data-driven sequencing of therapies. The goal is not simply regrowth; it is follicular preservation, inflammatory control, long-term stabilization, and aesthetic density optimization.
In my clinic, no two treatment plans are identical. Even patients with similar Norwood classifications can demonstrate dramatically different progression velocity, inflammatory burden, and response to therapy. Modern management is therefore algorithmic but individualized.
Advanced Follicular Biology: What We Understand in 2026
The hair follicle is now recognized as a highly dynamic mini-organ with immune privilege characteristics. In AGA, this immune privilege becomes partially disrupted.
Perifollicular Microinflammation
Scalp biopsies in progressive AGA frequently demonstrate:
– Mild lymphocytic infiltrates
– Increased prostaglandin D2 (PGD2) levels
– Oxidative stress markers
– Collagen deposition around follicles
This inflammatory microenvironment contributes to miniaturization. In 2026, anti-inflammatory modulation has become a secondary therapeutic pillar.
Stem Cell Niche Dysfunction
Bulge-area stem cells remain present even in advanced AGA, but their signaling capacity declines. This discovery reshaped treatment philosophy. The follicle is not destroyed it is suppressed.
Therapies now aim to reactivate dormant regenerative signaling rather than merely blocking hormones.
Advanced Pharmacologic Adjuncts
Low-Dose Oral Minoxidil (LDOM)
Low-dose oral minoxidil has gained substantial clinical acceptance. Unlike topical formulations, systemic administration improves adherence and ensures consistent follicular exposure.
Typical dosing range (2026 protocols):
– Men: 1.25–5 mg daily
– Women: 0.25–2.5 mg daily
Monitoring includes:
– Blood pressure assessment
– Baseline cardiovascular review
– Edema evaluation
In practice, I often see improved global density and reduced shedding within four months, particularly in patients who struggled with topical complianc.
Microneedling Protocols
Microneedling enhances transdermal delivery of topicals and stimulates wound-healing pathways linked to hair growth.
Standardized 2026 approach:
– Needle depth: 0.5-1.5 mm
– Frequency: Every 2-4 weeks
– Combined with topical growth stimulants
When combined with PRP or topical agents, synergistic outcomes are frequently observed.
Psychodermatology: The Emotional Component
Hair loss carries measurable psychological burden. Studies published between 2023–2025 confirm:
– Increased anxiety prevalence
– Higher rates of body image distress
– Social avoidance behavior
As clinicians, we address both biologic and psychological dimensions. Setting realistic expectations improves satisfaction and adherence.
I routinely schedule extended consultations for younger patients experiencing rapid progression. The reassurance provided during early intervention often changes long-term emotional outcomes.
Scalp Health Optimization
Inflammatory scalp conditions accelerate shedding. Antifungal shampoos containing ketoconazole (2%) are widely integrated into regimens.Ketoconazole also demonstrates mild antiandrogen properties at the follicular level.
Oxidative Stress Mitigation
Topical antioxidants and polyphenol-based serums are emerging adjuncts aimed at reducing reactive oxygen species in perifollicular tissue.
Long-Term Maintenance Strategy
AGA management requires a maintenance framework:
1. Initial stabilization (6–12 months)
2. Density optimization (12–24 months)
3. Long-term preservation phase
Stopping therapy typically results in gradual reversion to the natural progression pattern.
Special Populations
Young Men (Under 25)
Early intervention prevents extensive miniaturization. Conservative transplant planning is mandatory due to unpredictable long-term progression.
Aging Patients
Hair caliber naturally declines with age. Treatment intensity may be adjusted to reflect realistic density goals.- Stabilized frontal recession
Nutritional and Lifestyle Interventions
Iron and Ferritin
Ferritin levels below 40 ng/mL impair anagen maintenance. Supplementation protocols are individualized.
Vitamin D
Suboptimal vitamin D correlates with increased shedding. Correction improves follicular cycling stability.
Effective Medical Treatments for Hair Loss: Propecia, Proscar, and Avodart
Hair loss, particularly androgenetic alopecia, is a condition that affects millions of men worldwide. It is primarily driven by the hormone dihydrotestosterone (DHT), which causes hair follicles to shrink over time. To combat this, modern medicine has developed effective pharmacological interventions that target the 5-alpha reductase enzyme to inhibit DHT production.
The Power of Propecia in Hair Restoration
The most recognized name in this field is Propecia. Millions of men looking to buy an effective solution for receding hairlines or thinning crowns turn to this medication first. Propecia contains 1 mg of finasteride, a dosage specifically approved for treating male pattern baldness. When you decide to order your supply, it is essential to understand that Propecia works by significantly lowering scalp DHT levels, which helps stabilize hair loss and, in many cases, encourages regrowth. Many patients find that purchasing Propecia is the most reliable first step in their journey to restore hair density. Because it is the gold standard for long-term maintenance, many pharmacies facilitate the process of ordering Propecia online, though it should always be done under the guidance of a licensed healthcare professional.
Comparing Proscar and Avodart as Alternatives
While Propecia is the primary choice, other medications are often discussed in the same context. Proscar is another medication containing finasteride, but it is formulated at a higher dose (5 mg) and is typically indicated for the treatment of benign prostatic hyperplasia (BPH). Some patients who explore ways of purchasing cost-effective treatments may look into Proscar, though it is important to note that it is intended for prostate health. If you are considering buying this medication, you must consult a doctor, as it is not specifically marketed for hair loss at that dosage.
Another potent alternative is Avodart, which contains the active ingredient dutasteride. While Propecia inhibits one type of the 5-alpha reductase enzyme, Avodart is a dual-inhibitor, making it even more effective at reducing overall DHT levels. Although it is not officially FDA-approved for hair loss, many dermatologists consider ordering Avodart for patients who have not seen sufficient results with other treatments. Those interested in purchasing Avodart often do so as an “off-label” therapy for more aggressive hair loss.
Comparing Proscar and Avodart as Alternatives
Regardless of whether you choose to buy Propecia, Proscar, or Avodart, the key to success is consistency. Hair follicles respond slowly, and it often takes three to six months of daily use to notice a difference. Because these medications interact with your hormones, you should never attempt purchasing them from unverified sources. Always prioritize ordering from reputable, licensed pharmacies to ensure you are receiving genuine medication.
If you are just beginning to notice thinning, Propecia remains the most researched and widely accepted path forward. By ordering your treatment plan today, you are taking a proactive step toward maintaining your hair and boosting your confidence. Remember to always consult with a specialist before purchasing any of these prescriptions to ensure they are the right choice for your specific health profile.

FAQ:
Q.Its androgenetic alopecia permanent?
Yes, it is a chronic genetic condition, but progression can be slowed or stabilized with treatment.
Q.Can stress alone cause androgenetic alopecia?
Stress may accelerate shedding, but genetic androgen sensitivity drives AGA.
Q.Is low-dose oral minoxidil safe long term?
When prescribed and monitored appropriately, it is generally well tolerated.
Q.When should hair transplantation be considered?
After medical stabilization and when sufficient donor density exists.
Final Clinical Perspective
Androgenetic alopecia in 2026 is managed through integration: hormonal modulation, regenerative stimulation, advanced imaging, and surgical precision when indicated. Androgenetic alopecia in 2026 is managed through integration: hormonal modulation, regenerative stimulation, advanced imaging, and surgical precision when indicated. The earlier the intervention, the greater the likelihood of follicular recovery.
Hair biology is dynamic. With disciplined, individualized treatment strategies and continuous monitoring, long-term stability and visible density improvement are achievable for most patients.
Authoritative Sources
1. International Society of Hair Restoration Surgery (ISHRS) 2026 Guidelines
2. Journal of the American Academy of Dermatology (JAAD), 2025–2026 updates
3. PubMed Central: Androgenetic Alopecia Molecular Pathways Reviews
4. American Academy of Dermatology (AAD) Clinical Practice Guidelines 2026 .
2 thoughts on “ Advanced Clinical Strategies for Androgenetic Alopecia”